BOSTON — A team at Children’s Hospital of Philadelphia (CHOP) led by Rebecca Ahrens-Niklas, MD, PhD, and Lindsey George, MD, has described a case of a brain tumor linked to a rare integration of adeno-associated virus (AAV).
George presented the work at the American Society of Gene and Cell Therapy (ASGCT) conference in a plenary talk selected as the “presidential abstract” by ASGCT president, Terry Flotte, MD. The study, “Neuroepithelial tumor with AAV integration after intracisternal magna vector delivery,” was published in the New England Journal of Medicine.
Lindsey George, MD
Over the past 25 years, some 6,000 patients have been treated with some form of AAV gene therapy. In all that time, George said, there have been no established long-term safety concerns, although genome integration events have been reported in mouse and dog studies. But the case documented by George and colleagues at CHOP suggests that the gene therapy field may need to pay more attention to this potential occurrence.
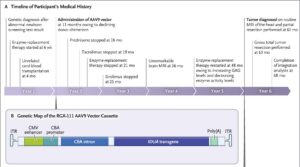
The story began with a 5-year-old boy with an inherited lysosomal disorder, severe MPS1 deficiency (Hurler subtype). The patient received enzyme replacement therapy at six weeks of age, followed by a cord blood stem cell transplant at age four months.
Investigators chose to perform gene therapy when the patient was 13 months old to deliver the iduronidase (IDUA) gene. The vector chosen was an AAV9 serotype, using a cytomegalovirus enhancer and a chicken beta-actin promoter driving the gene. The virus was administered into the boy’s cisterna magna in the base of the skull.
When the boy was five years old, a routine neurological scan revealed a large intraventricular mass that had not been observed two years earlier. Analysis of the tumor revealed it was a PLAG1-driven neuroepithelial tumor—indeed, PLAG1 expression was almost 300 times higher than in other central nervous system tumors studied at CHOP. (PLAG1 is usually only expressed during embryogenesis.)
Surgery to remove the tumor was successful. Eight months after surgery, there are no signs of tumor growth. The boy is also showing advanced neurocognitive function.
Tumor typing
George described RNA sequencing of the tumor, which revealed the fusion of a fragment of the AAV9 vector cassette to exon 5 of the PLAG1 gene on chromosome 8. The resulting transcript is predicted to encode a PLAG1 derivative containing five zinc-finger DNA-binding domains and a C-terminal transcriptional activation domain, which was previously reported to function as a transcriptional activator.
Credit: Dr_Microbe / iStock / Getty Images Plus
Curiously, the chimeric junction also included a segment of human chromosome 10, which George suspects originated during the vector manufacturing process. The integration event was present in about 40% of the total reads, suggesting integration into one of the two PLAG1 alleles.
George concluded her talk by noting that while the clinical outcome in this patient is so far encouraging, this is evidence that AAV integration can be associated with oncogenesis. The study underscores the need to monitor the most heavily transduced tissues after AAV gene therapy.
While the gene therapy community should be cautious in extrapolating this single case report across all AAV gene therapy programs, George said the study supports the use of the lowest feasible vector dose as well as tissue-specific promoters.
George noted that detection of the integrated AAV vector DNA was challenging, in part because of rearrangements of vector DNA. The use of several complementary techniques—long-read DNA sequencing, targeted PCR amplification, and RNA sequencing—was required to confirm the integration.
George and coworkers closed their paper, noting that, “Our findings support the hypothesis that rare AAV integration can contribute to human oncogenesis, which emphasizes the need to optimize gene delivery methods and monitor transduced tissues after treatment.”
BackgroundThe increasing demand for adult attention-deficit hyperactivity disorder (ADHD) assessments has required the development of efficient triage pathways. This study provides a formal assessment of a criterion-based screening model designed to prioritise patient safety and operational efficiency within a National Health Service (NHS) specialist secondary care setting.MethodsA prospective observational validation design was employed, involving 49 consecutive adults referred for ADHD assessment none of whom had a previous ADHD diagnosis. The Comprehensive ADHD Screening Questionnaire (CASQ), a clinician-administered instrument based on DSM-5 criteria, was utilised by four trained Physician Assistants. To ensure an assessment of triage safety, a universal assessment model was adopted: all participants received a blinded, gold-standard diagnostic assessment (NICE-compliant) regardless of the initial triage recommendation thereby eliminating verification bias. The primary outcome measure was the Number Needed to Harm (NNH), defined as the number of people screened before a single false-negative result occurs.ResultsOf the 48 participants who completed the diagnostic process, six (12.5%) received an ADHD diagnosis. The triage pathway correctly identified all six cases, resulting in a sensitivity of 100.0% (95% CI: 61.0%–100.0%) and an infinite NNH. Specificity was 45.2% (95% CI: 31.2%–59.9%), with a positive predictive value of 20.7%. The pathway permitted 39.6% (n = 19) of referrals to be triaged to alternative pathways rather than full ADHD assessment, potentially saving significant specialist clinician time. Exploratory analyses indicated that score magnitude did not reliably distinguish between true and false positives within the group triaged as appropriate for further assessment.ConclusionsThese preliminary findings suggest that criterion-based screening conducted by appropriately trained non-specialist clinicians can achieve high levels of safety whilst improving service efficiency. The findings support the feasibility of task-shifting models in adult ADHD services, provided that triage thresholds are calibrated to prioritise sensitivity. These results require replication in adequately powered multi-site studies before firm conclusions regarding pathway safety can be drawn. Further research is required to establish inter-rater reliability and cost-effectiveness across diverse clinical settings.
<strong>Background:</strong> Digital mental health interventions (DMHIs) have been widely promoted to improve access to mental health care within the UK National Health Service (NHS), particularly following the COVID-19 pandemic. In 2015, a total of 48 technologies were reportedly used in NHS services in England, but over the past decade, substantial changes to regulatory requirements, evidence standards, and procurement processes have reshaped the digital mental health landscape. There is limited clarity regarding which DMHIs are currently being formally procured and funded by NHS mental health services across the United Kingdom. <strong>Objective:</strong> This study aimed to identify and describe the DMHIs currently procured, contracted, or paid for by NHS mental health service providers in England, Scotland, and Wales for adult common mental health problems and to compare current procurement practices with findings reported in 2015. <strong>Methods:</strong> Freedom of Information requests were submitted to all NHS mental health trusts in England and all health boards in Scotland and Wales. Responses were collated and screened to provide an updated and extended record of which technologies are reportedly procured or paid for by services. <strong>Results:</strong> In total, 19 different DMHIs were identified as being procured across mental health service providers for adult common mental health problems at the time of data collection. This demonstrates a substantial reduction in the number of technologies being adopted into practice compared to the 48 reported in England in 2015. The findings reveal several key insights, including that only 2 technologies have remained in use for a decade, and they shed light on the types of technologies being selected and the variations in procurement practices among the 3 national health services. <strong>Conclusions:</strong> Despite the expansion of the digital mental health marketplace, the number of DMHIs formally procured by NHS mental health services has markedly decreased over the past decade. This consolidation may reflect increased selectivity and the adoption of higher-quality products, driven by strengthened regulatory oversight, evidence standards, and national guidance. Although these developments may enhance safety and quality assurance, they also raise important questions about innovation, market sustainability, and equitable access to digital mental health care. Ongoing monitoring of procurement practices is needed to inform policy, service design, and the future development of DMHIs.
Researchers have found that a retina that is aging faster than usual can indicate a lower bone density and an increased risk of fractures due to osteoporosis. Published today in PLOS Digital Health, these findings set the basis for a novel diagnostic method for a condition that remains underdiagnosed due to a lack of accessible screening tools.
“Osteoporosis is a common condition that weakens bones and raises the risk of fractures, especially in older adults,” write the study authors, who were led by Ching-Yu Cheng, MD, PhD, professor at the Duke-NUS Medical School and director of the Singapore Epidemiology of Eye Diseases (SEED) program. “However, many individuals are not diagnosed until after a fracture occurs, in part because the standard diagnostic test, dual-energy X-ray absorptiometry (DEXA), is not always readily accessible.”
A DEXA scan uses very low levels of X-ray radiation to measure a patient’s bone density—a major indicator of osteoporosis and fracture risk. However, it is a costly procedure requiring specialized equipment, and therefore typically only recommended for high-risk individuals with suspected fractures on X-rays or patients on long-term steroid therapy. This limits early detection in the broader population, with many people being diagnosed with osteoporosis only after experiencing a fracture.
Worldwide, nearly 20% of the population is affected by osteoporosis. If left untreated, this condition increases the risk of major fractures, which can be life-threatening and represent a large economic burden for healthcare providers. This drives an urgent need for accessible and non-invasive screening methods that can replace traditional DEXA scans.
Cheng’s team investigated whether images from a patient’s retina could help identify those at a higher risk of developing osteoporosis. This idea stemmed from previous research indicating that the retina can reflect the body’s overall biological aging.
The researchers developed a deep learning algorithm, known as RetiAGE, which calculates the probability of a person being older than 65 years based on images from their retina. They then investigated whether there was an association between RetiAGE results and bone mineral density (BMD) scores, as well as osteoporotic and hip fracture risk scores calculated using the fracture assessment tool (FRAX).
Retinal images and DEXA measurements were obtained from 1,965 participants in the PopulatION HEalth and Eye Disease PRofilE in Elderly Singaporeans (PIONEER) study. In this patient population, older RetiAGE scores were linked to lower BMD scores and an increased risk of major osteoporotic and hip fractures.
The ability of RetiAGE to predict the onset of osteoporosis was then evaluated in another 43,938 participants from a prospective UK Biobank cohort with retinal photographs and no osteoporosis at the time of taking these images. Higher RetiAGE scores, indicating accelerated retinal biological aging, were able to predict future osteoporosis onset even when adjusting for common osteoporosis risk factors as well as female-specific risks such as menopause and hormone replacement therapy.
“These findings suggest that retinal biological aging may reflect broader aging processes related to skeletal health,” state the researchers. “Retinal imaging may therefore provide a simple, non-invasive, and accessible way to support opportunistic screening for osteoporosis risk.”
IntroductionIrritable bowel syndrome (IBS) is a common gut-brain axis disorder characterized by abdominal pain and altered bowel habits, and it shows high comorbidity with psychiatric disorders. However, the shared genetic mechanisms underlying these associations remain incompletely understood.MethodsWe performed a large-scale meta-analysis of IBS in individuals of European ancestry by integrating genome-wide association study (GWAS) summary statistics from the UK Biobank, Bellygenes, and the Million Veteran Program (MVP), thereby increasing statistical power to detect novel IBS loci. We further conducted global genetic correlation analyses with psychiatric traits, followed by multi-trait analysis of GWAS (MTAG) and conditional false discovery rate (condFDR) analyses to identify pleiotropic loci. Transcriptomic, methylomic, and expression quantitative trait locus (eQTL) data were integrated to explore potential regulatory mechanisms.ResultsThe meta-analysis identified up to ten previously unreported IBS loci, several of which were supported by colonic and brain eQTL effects. Global genetic correlation analyses confirmed substantial genetic overlap between IBS and psychiatric traits, particularly major depressive disorder and neuroticism. MTAG and condFDR analyses uncovered more than 100 pleiotropic loci, including signals at SORCS1, SLC35D1, COA1, and TLE1. Integrative analyses of transcriptome- and methylome-wide data highlighted regulatory mechanisms spanning colonic, immune, and neuronal tissues, supporting neuro-immune crosstalk and mitochondrial involvement.DiscussionOur findings provide a comprehensive genetic characterization of IBS, refine its heritable basis, reveal pleiotropic links with psychiatric disorders, and implicate molecular pathways across the gut-brain axis. These results advance mechanistic understanding of IBS and may inform future therapeutic development for IBS and its psychiatric comorbidities.
When Jennifer got a job doing research for a nonprofit in 2023, she ran her new professional headshot through a facial recognition program. She wanted to see if the tech would pull up the porn videos she’d made more than 10 years before, when she was in her early 20s. It did in fact return some of that content, and also something alarming that she’d never seen before: one of her old videos, but with someone else’s face on her body.
“At first, I thought it was just a different person,” says Jennifer, who is being identified by a pseudonym to protect her privacy.
But then she recognized a distinctly garish background from a video she’d shot around 2013, and she realized: “Somebody used me in a deepfake.”
Eerily, the facial recognition tech had identified her because the image still contained some of Jennifer’s features—her cheekbones, her brow, the shape of her chin. “It’s like I’m wearing somebody else’s face like a mask,” she says.
“It’s like I’m wearing somebody else’s face like a mask.”
Conversations about sexualized deepfakes—which fall under the umbrella of nonconsensual intimate imagery, or NCII—most often center on the people whose faces are featured doing something they didn’t really do or on bodies that aren’t really theirs. These are often popular celebrities, though over the past few years more people (mostly women and sometimes youths) have been targeted, sparking alarm, fear, and even legislation. But these discussions and societal responses usually are not concerned with the bodies the faces are attached to in these images and videos.
As Jennifer, now 37 and a psychotherapist working in New York City, says: “There’s never any discussion about Whose body is this?”
For years, the answerhas generally been adult content creators. Deepfakes in fact earned their name back in November 2017, when someone with the Reddit username “deepfakes” uploaded videos showing faces of stars like Scarlett Johansson and Gal Gadot pasted onto porn actors’ bodies. The nonconsensual use of their bodies “happens all the time” in deepfakes, says Corey Silverstein, an attorney specializing in the adult industry.
But more recently, as generative AI has improved, and as “nudify” apps have begun to proliferate, the issue has grown far more complicated—and, arguably, more dangerous for creators’ futures.
Porn actors’ bodies aren’t necessarily being taken directly from sexual images and videos anymore, or at least not in an identifiable way. Instead, they are inevitably being used as training data to inform how new AI-generated bodies look, move, and perform. This threatens the livelihood and rights of porn actors as their work is used to train AI nudes that in turn could take away their business. And that’s not all: Advancements in AI have also made it possible for people to wholly re-create these performers’ likenesses without their consent, and the AI copycats may do things the performers wouldn’t do in real life. This could mean their digital doubles are participating in certain sex acts that they haven’t agreed to do, or even that they’re perpetrating scams against fans.
Adult content creators are already marginalized by a society that largely fails to protect their safety and rights, and these developments put them in an even more vulnerable position. After Jennifer found the deepfake featuring her body, she posted on social media about the psychological effects: “I’ve never seen anyone ask whether that might be traumatic for the person whose body was used without consent too. IT IS!” Several other creators I spoke with shared the mental toll that comes with knowing their bodies have been used nonconsensually, as well as the fear that they’ll suffer financially as other people pirate their work. Silverstein says he hears from adult actors every day who “are concerned that their content is being exploited via AI, and they’re trying to figure out how to protect it.”
One law professor and expert in violence against women calls these creators the “forgotten victims” of NCII deepfakes. And several of the people I spoke with worry that as the US develops a legal framework to combat nonconsensual sexual content online, adult actors are only at risk of further injury; instead of helping them, the crackdown on deepfakes may provide a loophole through which their content and careers could be stripped from the internet altogether.
How deepfakes cause “embodied harms”
During his preteen years in the 1970s, Spike Irons, now a porn actor and president of the adult content platform XChatFans, was “in love” with Farrah Fawcett. Though Fawcett did not pose nude, Jones managed to get his hands on what looked like pictures of her naked. “People were cutting out faces and pasting them on bodies,” Irons says. “Deepfakes, before AI, had been going around for quite a while. They just weren’t as prolific.”
The early public internet was rife with websites capitalizing on the idea that you could use technology to “see” celebrities naked. “People would just use Microsoft Paint,” says Silverstein, the attorney. It was a simple way to mash up celebrities’ faces with porn.
People later used software like Adobe After Effects or FakeApp, which was designed to swap two individuals’ faces in images or videos. None of these programs required serious expertise to alter content, so there was a low barrier to entry. That, plus the wealth of porn performers’ videos online, helped make face-swap deepfakes that used real bodies prevalent by the 2010s. When, later in the decade, deepfakes of Gal Gadot and Emma Watson caused something of a broader panic, their faces were allegedly swapped onto the bodies of the porn actors Pepper XO and Mary Moody, respectively.
But it wasn’t just high-profile actors like them whose bodies were being used. Jennifer was “a very minor performer,” she says. “If it happened to me, I feel like it could happen to anybody who’s shot porn.” Since he started his practice in 2006, Silverstein says, “numerous clients” have reached out to report “This is my body on so-and-so.”
Both people whose faces appear in NCII deepfakes and those whose bodies are used this way can feel serious distress. Experts call this type of damage “embodied harms,” says Anne Craanen, who researches gender-based violence at the UK’s Institute for Strategic Dialogue, an organization that analyzes extremist content, disinformation, and online threats.
The term reflects the fact that even though the content exists in the virtual realm, it can cause physiological effects, including body dysmorphia. The face-swapped entity occupies the uncanny valley, distorting self-perception. After discovering their faces in sexual deepfakes, many people feel silenced, experts told me; they may “self-censor,” as Craanen puts it, and step back from public-facing life. Allison Mahoney, an attorney who works with abuse survivors, says that people whose faces appear in NCII can experience depression, anxiety, and suicidal ideation: “I’ve had multiple clients tell me that they don’t sleep at night, that they’re losing their hair.”
Independent creators aren’t just “having sex on camera.” For someone to rip off their work “for their own entertainment or financial gain fucking sucks.”
Though the impact on people whose bodies are used hasn’t been discussed or studied as often, Jennifer says that “it’s just a really terrible feeling, knowing that you are part of somebody else’s abuse.” She sees it as akin to “a new form of sexual violence.”
The uncertainty that comes with not being aware of what your body is doing online can be highly unsettling. Like Jennifer, many adult actors don’t really know what’s out there. But some devoted followers know the actors’ bodies well—often recognizing tattoos, scars, or birthmarks—and “very quickly they bring [deepfakes] to the adult performer’s attention,” says Silverstein. Or performers will stumble upon the content by chance; some 20 years ago, for instance, the first such client to tell Silverstein her body was being used in a deepfake happened to be searching Nicole Kidman online when she found that one of the results showed Kidman’s face on her porn. “She was devastated, obviously, because they took her body,” he says, “and they were monetizing it.”
Otherwise, this imagery may be found by an organization like Takedown Piracy, one of several copyright enforcement companies serving adult content creators. US copyright violations can be challenging to prove if someone’s body lacks distinguishing features, says Reba Rocket, Takedown Piracy’s chief operating and marketing officer. But Rocket says her team has added digital fingerprinting technology to clients’ material to help flag and remove problematic videos, often finding them before clients realize they’re online.
By capturing “tens of thousands of tiny little visual data points” from videos, digital fingerprinting creates unique corresponding files that can be used to identify them, Rocket says—kind of like an invisible watermark. The prints remain even if pirates alter the videos or replace performers’ faces. Takedown Piracy has digitally fingerprinted more than half a billion videos and the organization has gotten 130 million copyrighted videos taken down from Google alone (though, of those videos, Rocket hasn’t tracked how many of these specifically include someone else’s face on a performer’s body).
Besides copyright, a range of legal tools can be used to try and combat NCII, says Eric Goldman, a law professor at Santa Clara University. For example, victims can claim invasion of privacy. But using these tools isn’t particularly straightforward, and they may not even apply when it comes to someone’s body. If there aren’t, for instance, unique markers indicating that a body in a deepfake belongs to the person who says it does, US law “doesn’t really treat [this content] as invasion of privacy,” Goldman says, “because we don’t know who to attribute it to.”
In a 2018 study that reviewed “judicial resolution” of cases involving NCII, Goldman found that one successful way plaintiffs were able to win cases was to assert “intentional affliction of emotional distress.” But again, that hinges on the ability to clearly identify the person in the content. Relevant statutes, he adds, might also require “intent to harm the individual,” which may be hard to show for people whose bodies alone are featured.
“AI girls will do whatever you want”
In the last few years, Silverstein says, it’s become less and less common to see the bodies of real adult content creators in deepfakes, at least in a way that makes them clearly identifiable.
Sometimes the bodies have been manipulated using AI or simpler editing tools. This can be as basic as erasing a birthmark or changing the size of a body part—minor edits that make it impossible to identify someone’s image beyond a reasonable doubt, so even porn actors who can tell that an altered image used their body as a base won’t get very far in the legal realm. “A lot of people are like, That looks like my body,” says Silverstein, but when he asks them how, they’ll reply, It just does.
At the same time, other users are now creating NCII with wholly AI-generated bodies. In “nudify” apps, anyone with a minimal grasp of technology can upload a photo of someone’s clothed body and have it replaced with a fake naked one. “So [much] of this content being created is just someone’s face on an AI body,” Silverstein says.
Such apps have drawn a ton of attention recently, from Grok “nudifying” minors to Meta running ads for—and then suing—the nudify app Crushmate. But there’s been relatively little attention paid to the content being used to train them. They almost certainly draw on the more than 10,000 terabytes of online porn, and performers have virtually zero recourse.
One reason is that creators aren’t able to demonstrate with any certainty that their content is being used to train AI models like those used by nudify apps. “These things are all a black box,” says Hany Farid, a professor at the University of California, Berkeley, who specializes in digital forensics. But “given the ubiquity” of adult content, he adds, it’s a “reasonable assumption” that online porn is being used in AI training.
“It’s just not at all difficult to come up with pornographic data sets on the internet,” says Stephen Casper, a computer science PhD student at MIT who researches deepfakes. What’s more, he says, plenty of shadowy online communities provide “user guides” on how to use this data to train AI, and in particular programs that generate nudes.
It’s not certain whether this activity falls within the US legal definition of “fair use”—an issue that’s currently being litigated in several lawsuits from other types of content creators—but Casper argues that even if it does, it’s ethically murky for porn created by consenting adults 10 years ago to wind up in those training data sets. When people “have their stuff used in a way that doesn’t respect or reflect reasonable expectations that they had at that time about what they were creating and how it would be used,” he says, there’s “a legitimate sense in which it’s kind of … nonconsensual.”
Adult performers who started working years ago couldn’t possibly have consented to AI anything; Jennifer calls AI-related risks “retroactively placed.” Contracts that porn actors signed before AI, adds Silverstein, might provide that “the publisher could do anything with the content using technology that now exists or here and after will be discovered.” That felt more innocuous when producers were talking about the shift from VHS to DVD, because that didn’t change the content itself, just the way it was conveyed. It’s a far different prospect for someone to use your content to train a program to create new content … content that could replace your work altogether.
Of course, this all affects creators’ bottom line—not unlike the way Google’s AI overviews affect revenue for online publishers who’ve stopped getting clicks when people are content with just reading AI-generated summaries. Performers’ “concern is … it’s another way to pirate [their] content,” says Rocket.
After all, independent creators aren’t just “having sex on camera,” as the adult content creator Allie Eve Knox says. They’re paying for filming equipment and location rentals, and then spending hours editing and marketing. For someone to then rip off and distort that content “for their own entertainment or financial gain,” she says, “fucking sucks.”
KIM HOECKELE
Tanya Tate, a longtime adult content creator, tells me about another highly unsettling AI-created situation: She was recently chatting with a fan on Mynx, a sexting app, when he asked her if she knew him. She told him no, and “his eyes just started watering,” Tate says. He was upset because he thought she did know him. Turns out he’d sent $20,000 to a scammer who’d used an AI-generated deepfake of Tate to seduce him.
Several men, Tate subsequently learned, had been scammed by an AI version of her, and some of them began blaming her for their losses and posting false statements about her online. When she reported one particularly aggressive harasser to the police, they told her he was exercising his “freedom of speech,” she says. Rocket, too, is familiar with situations where AI is used to take advantage of fans. “The actual content creator will get nasty emails from these people who’ve been scammed,” she says.
Other porn actors say they fear that their likenesses have been used without consent to do other things they wouldn’t do. One, Octavia Red, tells me she doesn’t do anal scenes, “but I’m sure there’s tons of deepfake anal videos of me that I didn’t consent to.” That could cost her, she fears, if viewers choose to watch those videos instead of subscribing to her websites. And it could cause fans to develop false expectations about what kind of porn she’ll create.
“I saw one AI creator saying, ‘Well, AI girls will do whatever you want. They don’t say no,’” says Rocket. “That horrifies me … especially if they’re training those AI models on real people. I don’t think they understand the damage to mental health or reputation that that can create. And once it’s on the internet, it’s there forever.”
Efforts to “scrub adult content from the internet”
As AI technology improves, it’s increasingly difficult for people to discern any type of real video from the best AI-generated ones on their own. In one 2025 study, UC Berkeley’s Farid found that participants correctly identified AI-generated voices about 60% of the time (not much better than random chance), while advances like false heartbeats make AI-generated humans tougher than ever to spot.
Nevertheless, most lawyers and legal experts I spoke with said copyright laws are still adult performers’ best bet in the US legal system, at least for getting their face-swapped content taken down. For his clients, Silverstein says, he tries to figure out the content’s origins and then issue takedown requests under the Digital Millennium Copyright Act, a 1998 law that adapted copyright law for the internet era. “Even recently, I had a performer who has an insanely well-known tattoo,” he says, and with a DMCA subpoena he managed to identify the poster of the content, who voluntarily removed it.
But this way of working is becoming increasingly rare.
These days it’s nearly “impossible,” Silverstein says, to determine who produced a deepfake, because many platforms that host pirated content operate facelessly. They’re also often based in places that “don’t really care about US law when it comes to copyrights,” says Rocket—places like Russia, the Seychelles, and the Netherlands.
While governments in the EU, the UK, and Australia have said they will ban or restrict access to nudify apps, it’s not an easily executed proposition. As Craanen notes, when app stores remove these services, they often simply reappear under different names, providing the same services. And social platforms where people share NCII deepfakes, argues Rocket, are slacking in getting them removed. “It’s endless, and it’s ridiculous, because places like Twitter and Facebook have the same technology we do,” Rocket says. “They can identify something as an infringement instantly, but they choose not to.”
(Apple spokesperson Adam Dema emailed, “’nudification’ apps are against our guidelines” in the app store, and it has “proactively rejected many of these apps and removed many others,” flagging a reporting portal for users. A Google spokesperson emailed, “Google Play does not allow apps that contain sexual content,” noting it takes “proactive steps to detect and remove apps with harmful content” and has suspended hundreds of apps for violating its policy. Meta spokesperson shared a blog post about actions it’s taken against nudify apps, but did not respond to follow-up questions about copyrighted material. X did not respond to a request for comment.)
As porn performers are forced to navigate AI-related threats, the only current federal law to address deepfakes may not help them much—and could even make matters worse. The Take It Down Act, which became US law last year, criminalizes publishing NCII and requires websites to remove it within 48 hours. But, as Farid notes, people could weaponize the measure by reporting porn that was made legally and with consent and claiming that it’s NCII. This could result in the content’s removal, which would hurt the performers who made it. Santa Clara’s Goldman points to Project 2025, the Heritage Foundation’s policy blueprint for the second Trump administration, which aims to wipe porn from the web. The Take It Down Act, he argues, “allows for the coordinated effort to scrub adult content from the internet.”
US lawmakers have a history of hurting sex workers in their attempts to regulate explicit content online. State-level age verification laws are an example; visitors can pretty easily get around these measures, but they can still result in reduced revenue for adult performers (because of lower traffic to those sites and the high price of age-checking services they have to purchase).
“They’re always doing something to fuck with the porn industry, but not in a way that actually helps sex workers,” says Jennifer. “If they do something, they’re taking away your income again—as opposed to something like giving you more rights to your image, [which] would be tremendously helpful.”
But as generative AI plays an increasingly large role in NCII deepfakes, the types of images to which adult performers have rights moves deeper into a gray area. Can actors lay claim to AI images likely trained on their bodies? How about AI-generated videos that impersonate them, like the one that tricked Tanya Tate’s fan?
The biggest challenge will be creating “legitimate, effective laws that will absolutely protect content creators from abusing their likeness to train and create AI,” Rocket says. “Absent that, we’re just going to have to keep pulling content down from the internet that’s fake.”
In the meantime, a few porn actors tell me, they’re trying to take advantage of copyright laws that weren’t really made for them; they’ve signed with platforms that host their AI-generated duplicates, with whom fans pay to chat, in part so they’ll have contracts that protect ownership of their AI likenesses. When I spoke with the actor Kiki Daire in September 2025 for a story on adult creators’ “AI twins,” she said she “own[ed] her AI” because she’d signed a contract with Spicey AI, a site that hosted AI duplicates of adult performers. If another company or person created her AI-generated likeness, she added, “I have a leg to stand on, as far as being able to shut that down.”
Even this, though, is not a sure thing; Spicey AI, for instance, shut down several months after I spoke with Daire, so it’s unlikely that her contract would hold. And when I spoke in October with Rachael Cavalli, another adult actor who had signed with an AI duplicate site in hopes it’d help protect her AI image, she admitted, “I don’t have time to sit around and look for companies that have used my image or turned something into a video that I didn’t actually do … it’s a lot of work.” In other words, having rights to your AI image on paper doesn’t make it easier to track down all the potentially infinite breaches of those rights online.
If she’d known what she knows about technology today, Jennifer says she doesn’t think she would have done porn. The risks have increased too much, and too unpredictably. She now does in-person sex work; it’s “not necessarily safer,” she says, “but it’s a different risk profile that I feel more equipped to manage.”
Plus, she figures AI is unlikely to replace in-person sex workers the way it could porn actors: “I don’t think there’s going to be stripper robots.”
Jessica Klein is a Philadelphia-based freelance journalist covering intimate partner violence, cryptocurrency, and other topics.
President of the American Society of Gene and Cell Therapy (ASGCT), Terry Flotte, MD, is excited to host this year’s conference in his own backyard. It will be a short drive east on the Mass Turnpike from his office at UMass Chan Medical School in Worcester to the Menino Convention and Exhibition Center in Boston’s Seaport district. Flotte is hopeful that the 2026 conference will draw the largest attendance in the meeting’s history. His tenure as president ends this week on the last day of the conference, May 15.
In the run-up to this year’s conference, GEN spoke with Flotte, who is also Editor in Chief of GEN’s sister journal Human Gene Therapy, about the central themes and most anticipated sessions at this year’s conference. “I have a full dance card, let me tell you,” Flotte joked. The conference will highlight several themes of Flotte’s productive tenure.
(This interview has been edited for length and clarity.)
GEN:Terry, what’s the theme of this year’s ASGCT conference?
Terry Flotte: We’re working very hard on access for rare and ultra-rare conditions and have been for some time. You’ll see that in the presidential symposium. This is in the context of our mission to improve access to rare disease cell and gene therapy (CGT). This is the guiding principle of our strategic plan: we want to work for universal access to CGT. There are two orthogonal axes to this: I’m focusing on rare and ultra-rare diseases. ASGCT is going to continue to work in parallel on universal access in a more global context.
We have created a first-of-its-kind exchange for shelved CGTs. An increasing number of CGTs for rare and ultra-rare diseases are being discontinued or deprioritized after they reach the clinical stage—not because they lack clinical efficacy but because they lack market viability. We have partnered with Orphan Therapeutics Accelerator to create a new entity called CGTxchange. This collaborative venture is meeting the need of these promising clinical-stage CGTs that are not progressing. This entity will be an AI-enabled digital platform that will list the available clinical-stage CGT programs and generate AI-enhanced profiles, digest the data, score them for their level of advancement and the robustness of their responses, and essentially shorten the due diligence that investors normally have to do, enabling the connections to work faster.
I estimate there’s at least 50-100 of these programs. We had our own personal experience with Sio Gene Therapies [formerly Axovant] on both GM1 and GM2 gangliosidosis. This is part of a broader set of initiatives. Over the past few years, we created a taskforce in response to this increasing rate of discontinuation of these therapies. The two main outgrowths that the ASGCT board has endorsed are to create a consortium of CGT developers that might be able to offer non-profits less expensive manufacturing in a limited way but also work toward a drug master file sharing data for those who benefit from the less expensive vectors—in addition to the clearinghouse I just mentioned.
GEN: What else is new this year?
Flotte: A new thing for ASGCT is we’re having a patient advocate presenting. Terry Pirovolakis pioneered the CGT therapy for spastic paraplegia type 50 (SPG50) by developing his own company, Elpida Therapeutics, which has taken SPG50 to the clinic and now is doing that for other rare and ultra-rare diseases.
The second example is from Claire Booth, MBBS, PhD, (Great Ormond Street Children’s Hospital, London). Her team has received market authorization to be the
pseudo-commercial manufacturer of a fully licensed therapeutic for different forms of SCID.
Those are two direct examples of alternatives to get things to the clinic, other than getting a new commercial sponsor. [Hopefully] we can end up getting more of those picked up, whether through the CGTxchange or direct outreach. We’re also going to honor Timothy Yu, MD, PhD, with the Jerry Mendell Translational Research Award. He will be talking about the N=1 Collaborative with the parallel effort with oligonucleotide therapeutics. There is a purposeful theme to this meeting, aiming to make a big change in how things can get to the clinic and stay in the clinic.
GEN: Last year in New Orleans, the conference was dominated by the Baby KJ story. Will anything stand out in the same way this year?
Flotte: We are honoring the three primary authors of the Baby KJ story—Kiran Musunuru, MD, PhD, Rebecca Ahrens-Niklas, MD, PhD, and Fyodor Urnov, PhD.
I have also selected the work of Lindsey George, MD (Children’s Hospital of Philadelphia) as a presidential abstract. She is going to present the first case of an AAV-induced tumor—or at least an aggressive and autonomously growing malignancy…. This occurred in an MPS1 patient who received a high dose of AAV into the ventricles. It is not exactly a meningioma, but it’s arising from the neuroepithelial cells lining the ventricles. The tumor has AAV integrated with a strong promoter immediately upstream of a known oncogene. I put that into the presidential lecture, even though it’s not good news—but I’m not a [gene therapy] campaign manager here! I think this is a significant finding that we’ll have to pay attention to.
Lindsey is not saying that nobody should ever do this again. She’s going to point out aspects of this that were very manageable and how this patient overall has a dramatically better outcome than they would have without the therapy. In a way, [this is] somewhat like when those leukemia cases developed in Europe in the early SCID [gene therapy] trials. It is in a way parallel to that.
GEN: This will be your last conference as president of ASGCT!
Flotte: Yes, it ends on May 15th! We only get to be president for one year. I started the Rare Disease Task Force as vice president. This was my cause over the past three years [as an officer]. I’m very pleased we were able to stand this up.
We have an actual corporation, a joint venture, 50% owned by ASGCT. We set up this manufacturing consortium. Somewhat related, we set up our own charitable foundation, the ASGCT Foundation. We will have our first event—a gala at the conference. It will have a lot of time to grow. The foundation has just been incorporated as a subsidiary not-for-profit.
GEN: How do you view things at FDA currently?
Flotte: We will have a fireside chat with the new director of CBER, Katherine Szarama, PhD. We are very encouraged—she’s a very highly trained professional. We love that FDA is paying a lot of attention to rare diseases, but we need some scientific and evidence-based guidelines on how to do this consistently. We’re looking to someone who has regulatory experience.
GEN: What else has got you and your colleagues in the gene therapy space excited of late?
Flotte: I’m hoping we’re going to better understand high-dose AAV toxicity… I think what we’ve got is several different syndromes, but many of them may have a common link… We’ve been seeing with high-dose AAV a very broad distribution, but the doses are incredibly high and there have been deaths—the DMD patient deaths that occurred in the first two weeks are the best-known examples, but there have been other ones.
In my lab, we’re trying to figure out the primary pathogenesis. We have found a number of situations with unexpected vector expression in the endothelial cells and then seeing vascular leakage into some of these tissues causing tissue injury. So, in the post-mortem analysis we helped on, we saw high expression in the lungs and alveolar capillaries. They had diffuse leakage into the capillaries leading to a syndrome known as acute respiratory distress syndrome (ARDS). But in some of the others where they’re seeing some complement activation, we think that small vessel injury could be a convergent pathway. Now, where does this come into play in the broader sense?
One of the holy grails of recent AAV gene therapy is to design an AAV capsule that efficiently crosses the blood-brain barrier. Many diseases that are appropriate for AAV are diseases of the central nervous system (CNS). You can think of, for instance, the easiest cells to access in the CNS are the spinal motor neurons, hence the SMA1 treatment, Zolgensma. So, if you treat an SMA newborn, that is essentially solved or at least adequately solved. But in none of the diseases that affect the brain have we seen an IV gene therapy that is robustly efficacious—just giving an AAV at a high enough dose to get across the blood-brain barrier. Many different companies are trying to develop AAV capsids that will penetrate the blood-brain barrier, the first one that got to clinic was a vector designed by Capsida Biotherapeutics. But the first patient treated on the Capsida trial developed cerebral edema and died.
One of the important challenges for the field is to understand if we can separate a blood-brain barrier penetration from endothelial cell toxicity, because you could think perhaps a vector designed to get through the blood-brain barrier could cause injury as it crosses to the endothelial cells in the brain. I think there may be ways around this, but to me this is a central issue because the CNS is affected in so many single-gene disorders. The parents see a child who has a disability or degenerating, as in Tay-Sachs, and they want to be able to do an IV therapy. They don’t want to have to have a direct brain injection or some other invasive intervention. So that’s what I’m looking for at ASGCT 2026.
Choosing the right additives could help “cell-free” expression systems finally fulfill their potential and provide biopharma with a low-cost way of making protein drugs, according to a recent research report.
The new study looked at how cell-free systems, in which biochemical reactions occur independently of cells, could be fine-tuned to provide drug makers with alternatives for large-scale protein production.
And the potential of the approach is significant, says Karen Polizzi, PhD, a professor from the department of chemical engineering at Imperial College London, who adds, “Cell-free protein synthesis (CFPS) is a flexible manufacturing technology. It can be used for on-demand synthesis in low-resource environments or to make difficult-to-express products, especially medicines that are toxic to the cell. Cell-free reactions scale well across microliter to liter scale without needing adjustments.”
The Imperial team’s research focused on expression systems based on the yeast species Pichia pastoris, which, as Polizzi explains, “has machinery capable of post-translational modifications of proteins that can be necessary for function.”
As an expression host, P. pastoris combines elements of both prokaryotic and eukaryotic systems, such as a rapid growth rate and the ability to perform post-translational modifications (PTMs).
The problem is that current commercially available Pichia systems are only able to produce low amounts of protein. According to Polizzi and her co-authors, the productivity of P. pastoris-based cell-free systems usually ranges from 6 to 100 µg/mL, which is only approximately five percent of that achieved by comparable E. coli systems. In addition, the additives required by Pichia-based systems are more expensive than those required by equivalent platforms.
Additives to improve yields
To address this, Polizzi and co-authors systematically evaluated a variety of chemical additive combinations to identify the most effective stabilizers and crowding agents to be incorporated in the reaction.
The researchers also used a machine learning model to predict translation initiation rates and optimized the Kozak sequence—the protein translation initiation site in most eukaryotic mRNA transcripts—to enhance expression.
In addition, the Imperial team evaluated lower-cost glycolytic intermediates as substrates for ATP regeneration to reduce the cost of goods.
Polizzi says, “We focused on how to improve the yields and reduce the cost of production. We identified some additional additives that boost the yield without substantially increasing the cost. We also identified a different energy source that can be used.”
She adds, “This work underscores the importance of protein-stabilizing additives and the role of rationally designed DNA sequences with minimized mRNA structural complexity to enhance yield in CFPS. Our demonstration of glycolytic intermediates as a potential secondary energy system additionally provides the foundation for the development of a cost-effective P. pastoris CFPS.”
BOSTON – The annual American Society of Cell and Gene Therapy (ASGCT) conference got underway in Boston this week with a guest appearance by one of gene therapy’s greatest ambassadors and patient advocates.
Victoria Gray, the sickle cell warrior who was successfully treated in the exa-cel clinical trial sponsored by Vertex Pharmaceuticals/CRISPR Therapeutics seven years ago, spoke in an evening workshop organized by the Emily Whitehead Foundation and ScaleReady.
Boston is becoming a regular stomping ground for Victoria. Last November, she spoke at the Genetic Agency Technology Conference, hosted by Dyno Therapeutics. Last month, she finally received an invitation to visit the headquarters of Vertex and speak in a town hall meeting.
In an extemporaneous 20-minute speech, Victoria talked about her lifelong journey with sickle cell disease (SCD). She recalled her first major pain crisis, when she was a young girl—a lightning-type pain that began in one arm before traveling across her chest and down the other arm. “In minutes, my entire body was engulfed in pain,” she said. “The pain felt like getting struck by lightning and hit by a truck. It took me to the floor.” Her grandmother provided hot towels and Tylenol, but nothing worked—not even prayer. After a week in hospital, Victoria returned home but still felt fatigued.
Stricken by regular pain crises, a hallmark of SCD, Victoria encountered numerous disappointments growing up. Her hematologist said she could not join the cheer team. In eighth grade, she was told she could not join the basketball team, because the exertion would provoke a pain crisis. “As a kid, I was like a Timex: I could take a licking and keep on ticking,” she joked.
In high school, she signed up to join the United States Navy. “I wanted to serve my country,” Victoria recalled. As she was preparing for basic training, she learned that her disease prevented her from enrolling. “So that was another dream lost.” Next, she turned her attention to nursing. Victoria graduated high school in 2003, but it took another seven years before she could qualify for a nursing program. “Professors didn’t understand because I looked whole and complete. They didn’t think I was sick.”
In 2010, just before Halloween, Victoria had the worst pain crisis of her life, stripping her ability to walk or use her arms to feed herself. “I couldn’t do anything, facing some of the worst pain of my life. I was getting strong pain medicines like Dilaudid, ketamine, but still couldn’t move. Pain had taken over my thoughts.” Unable to sleep or even take a nap, Victoria was desperate to go home to her family.
Later, she asked the doctors if they had heard about a haplo-bone marrow transplant (BMT). “I can’t continue living like this,” she said. The doctors looked at each other and said no. After weeks of prayer, Victoria received a call from her hematologist. “Victoria, I have good news, but I only want to tell you in person.” For the first time in her adult life, Victoria was excited about a doctor’s appointment.
She traveled to Nashville with her brother, who would be her BMT donor, and her husband. She met Haydar Frangoul, MD, whom Victoria calls, “the nicest doctor that I’ve met in my adult life.” Frangoul told her: “Victoria, I wish I had met you ten years ago!’
Although Victoria’s brother was a suitable BMT match, Victoria was scared of the possibility of graft vs. host disease (GVHD). “My purple pill basket was filled to the brim with medicine every day. If I would acquire [GVHD], that basket would have to triple in size.”
“I’m a human!”
On her next visit to Nashville, she had to extend her stay because of another pain crisis. But that stay changed her life. Frangoul sat next to her bedside. “Victoria, have you ever heard of CRISPR?” he asked. Victoria shook her head.
Frangoul used a typo-in-a-textbook analogy and reassured Victoria that there was no chance of GVHD, because she would be receiving her own modified stem cells. “You’ll be the first person to do this, Victoria,” he said. “First human?” she asked. “Yes,” Frangoul said, “but it’s been tested in primates.”
“But I’m a human!” she said.
After being reassured that she could still try a bone marrow transplant if the procedure did not work, Victoria agreed to move forward. The chemotherapy, was “hell on Earth,” she recalled. “I lost my hair, which I was prepared for, but the mucositis, the sores in my mouth, the inability to eat for two weeks, was gruesome.”
Victoria swallowed her tears and decided to fight. This was the first time she had been in the hospital by her choice, to live for her children. About eight months after receiving her CRISPR-edited stem cells in July 2019, she woke up one morning, not feeling anything. “Oh my God, I’m dead,” she thought. She called her kids into the room and hugged them, slowly realizing that “this is what normal feels like.” For the first time in more than 25 years, Victoria did not have any pain in her lower back and hips. She was able to breathe deeply without wincing.
A few years after her therapy, Victoria was finally able to take her first ever flight, to Washington D.C. to visit her husband, who was on deployment. “It was the first time that I was ever able to show up for the man who has shown up for me,” she said. She has since watched her daughter dance in a Christmas parade and supported her son playing high school football. “The little things have brought me great joy,” she said.
Her second flight was a business class trip to London with her husband in March 2023, where she spoke at the third International Summit on Human Genome Editing. “I got to keep my covenant that I made with God, that God, if you do this for me, I would tell the world about what you did.”
Victoria welcomed her first granddaughter on Christmas Eve, 2024. Next week, another milestone: she will be in the audience as her twins graduate high school. And next month, she will publish a children’s book called Hema’s Journey, the tale of her inspiring journey with CRISPR gene therapy. She’s currently training for a group effort to climb Mt. Kilimanjaro.
Perhaps at next year’s ASGCT conference in Philadelphia, she will be invited to present in a plenary session on the main stage. It would be hard to think of a more fitting speaker.